Firstly, quick shout out to the team at Goose Chiropractic & wellbeing Clinic in Dinnginton for an excellent seminar on Saturday.
Great day of lectures to DC and CA’s alike.

If you missed the collagen seminar on Wednesday night, do not fret, below is the recording.
Passcode: cjAK=d2b
It runs approximately 40 minutes with lots of wide ranging Q&A’s at the end.
Now to everyones favourite primary prevention drug, statins.
Did you know that for many years it has been known that an increased level of inflammation is a risk factor for heart disease, strokes and indeed pretty much everything bad.
Hence, the term, inflamm-aging.

This was part of the huge study known as JUPITER.
Here is the background:
“Increased levels of the inflammatory biomarker high-sensitivity C-reactive protein predict cardiovascular events. Since statins lower levels of high-sensitivity C-reactive protein as well as cholesterol, we hypothesized that people with elevated high-sensitivity C-reactive protein levels but without hyperlipidemia might benefit from statin treatment.”
17, 802 people with LDL under 3.4 mmol/L, and CRP (marker of inflammation) over 2 mg/L.
KEY POINT
The NHS does not consider CRP to be high unless it is above 7.5 mg/L, occasionally 5 mg/L.
We consider anything over 1 mg/L as suboptimal and it is a spectrum up towards the “official” high, with risk of ill health creeping up as you go higher.

It is fascinating that the researchers paid by the pharmaceutical industry have read the literature and know all this, but the NHS guidance does not reflect this.
At least until they can get a drug to bring down inflammation and cut the risk of CVD, hence this study.
The question you could ask quite reasonably is why not utilise lifestyle to reduce inflammation, which is a symptom not a disease.
Elevated inflammation means your immune system is overactive, why?
The food you eat?

Infections in your gut?
Too much stress, not enough sleep?
Regardless, I find it incredible there are millions of people wandering around at risk of CVD via a sustained low grade inflammatory RESPONSE (a response to something or because of something, it is not an accident), and the NHS ignore it.
It is worth noting that the study did show a reduction in CVD, strokes, though this was a statistical difference between the drug and the placebo. 9.5 and 9.2 events per 100 patient years.
So while it might be statistically “significant”, in absolute terms it is meaningless.
Also, the secondary endpoint of all cause mortality, they found no difference at all.
Now the study only ran 1.9 years on average, which is not really long enough, so it may be that the longer the study, the bigger the benefits begin to get.
This is certainly the argument of some, but the issue is as the benefits for some increase, so do the side effects for others.
We cannot know who is going to get the benefit and who is not, that is the issue with primary prevention.
The vast majority of people in primary prevention (stopping the first event) are not going to have a coronary event, so the chances of success are always going to be minuscule.
Even secondary prevention studies with statins are increasingly finding zero benefits.

“Rosuvastatin did not reduce the primary outcome or the number of deaths from any cause in older patients with systolic heart failure”
Researchers looking for trends between statin use and coronary issues are not finding an association.
“Conclusions: Among the Western European countries studied, the large increase in statin utilisation between 2000 and 2012 was not associated with CHD mortality, nor with its rate of change over the years.”
Currently, we are at an all-time high prescription rate for statins/all time low holesterol rates and yet we are now seeing a comeback of CVD deaths after a long decline.

Check out this graph.
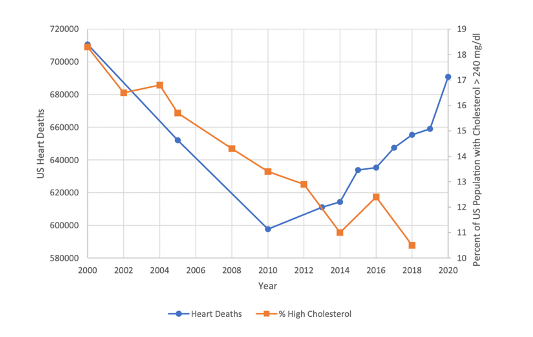
On this last point it is worth noting the graph ends in 2020, and since 2021 we have seen an explosion of heart attacks and strokes across all ages, 10-20% excess deaths occurring every month.