Before we get into today’s newsletter, did you know we have expanded our IN Health supplement website?
We now have the facility to send a recommended supplement/supplements directly from your account, to a patient for them to then make a purchase?
Click the star on the product image, and it goes into the “Recommended supplement” page.

Once into the recommended supplement section, either click the email icon which should link up with your email system automatically, or copy and paste the URL into an email with any instructions.
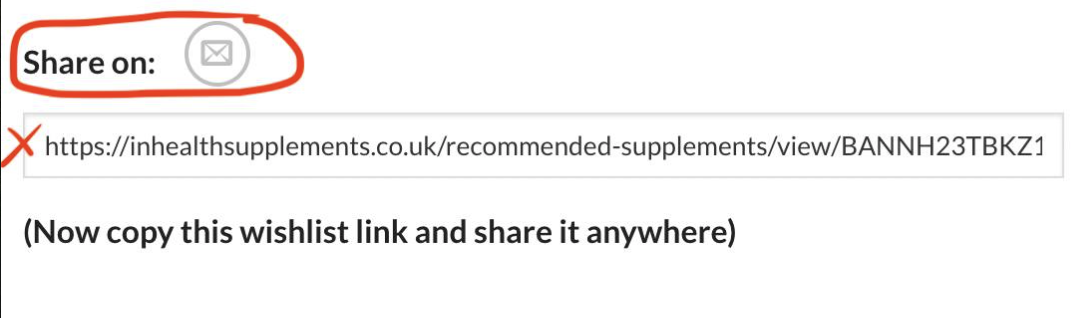
This really lowers the friction with an online sale if you are not holding stock in clinic.
You can see how it works in the 5 minute video below ????
Remember once a patient is registered under your account (you will get an email when they do that) then you get 20% commission on everything they order for life (and an email every time they place an order).
Note, once the patient is into the system, they now also have the opportunity to subscribe and save for monthly delivery with a 5% discount.
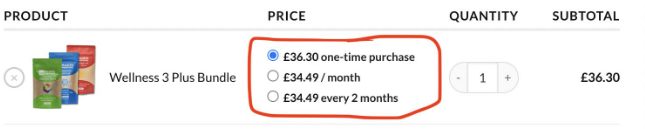
Note here, we also now have product bundles available, these are still being added, but there is the Daily Maintenance 2 (Vit D/K2 and Mag Duo Plus), Wellness 3/Wellness 3 PLUS, Core 4 PLUS Repair & Prevent.
FYI, when you see a bundle with a “PLUS” in the bundle name this indicates the MAGNESIUM product is the MAGNESIUM DUO PLUS which indicates it has 15 mg of B6 added to the same magnesium found in the regular MAGNESIUM DUO.
This makes it easy as it is one click for you and the client and one purchase.
We are also working on new bundles for migraine, B12 protocol and more.
In other news, I have had quite a few of you email me regarding a recent Zoe podcast with Tim Spector, the rheumatologist turned “health” expert via epidemiology.
Here is the truth about medics that start actually looking at health rather than disease, 99% of them just do not get “it”.
They end up playing medicine with diet & supplements, but cannot let go of the desire to use RCT’s to prove anything they do and ignore (or may be ignorant) of the basic science/biology of what they are studying.
I will not post a link to the actual video, it is that bad and if you do find it online, have some fun and check the comments section – they are getting hammered.




Even their viewers know more than they do about a systems biology approach.
They believe you do not need to take supplements, that you can use food and do not worry about the lack of sunlight in the winter.
The reason is really around their desire to have an RCT for condition X, Y or Z, with vitamin D only given and a big response.
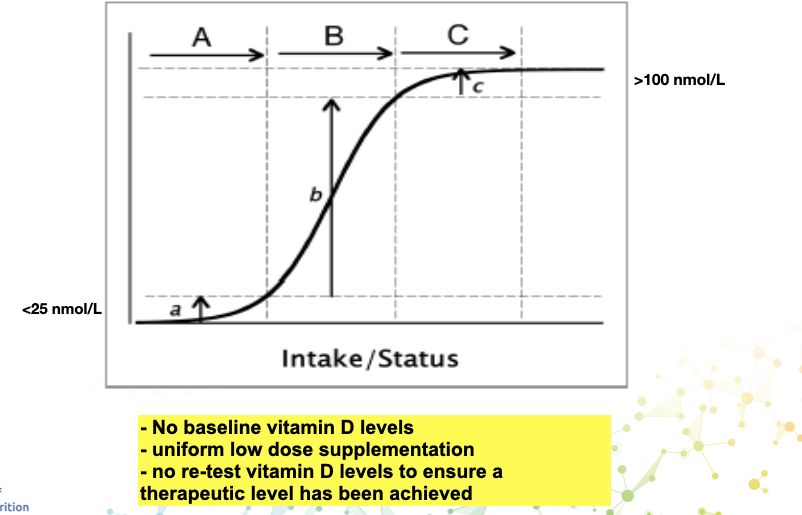
The issue is two fold, firstly, in the studies that are used in meta-analysis to produce Tim’s opinion, they often do not test the vitamin D blood levels (I am not making this up).
They will take a group of people of unknown vitamin D levels with a condition (let’s say depression), then they give a tiny dose, that will not get you out of deficiency if you are very low and certainly nowhere near optimal (we will discuss that later).
Then at the end of the study, the conclusion reads “vitamin D is ineffective in the treatment of depression”.
But the conclusion should really read, “non-physiological doses of vitamin D, in patients of unknown vitamin D status, is ineffective in the treatment of depression” – But we do not need a study to know that, it is a given, an a priori if you will.
Even if they had tested vitamin D and diagnosed deficiency but still gave an ineffective dose of vitamin D but failed to retest, they would not know they had failed to achieve optimal levels or at least failed to resolve deficiency.
Let me show you this in action.
I read an article with an unusual title:
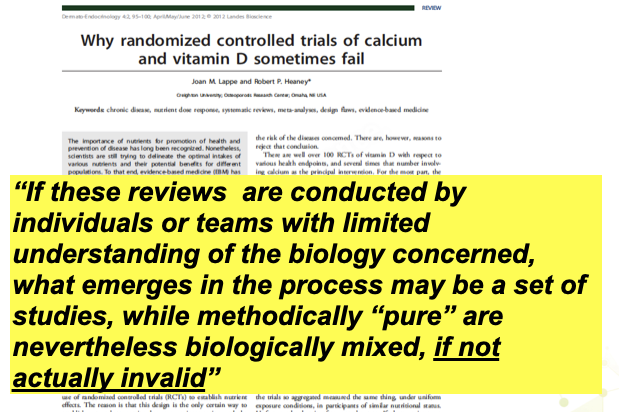
Vitamin D and depression: A systematic review and meta-analysis comparing studies with and without BIOLOGICAL FLAWS.
What, I wondered, did the “biological flaws” relate to?
Well, it leads me to another article.
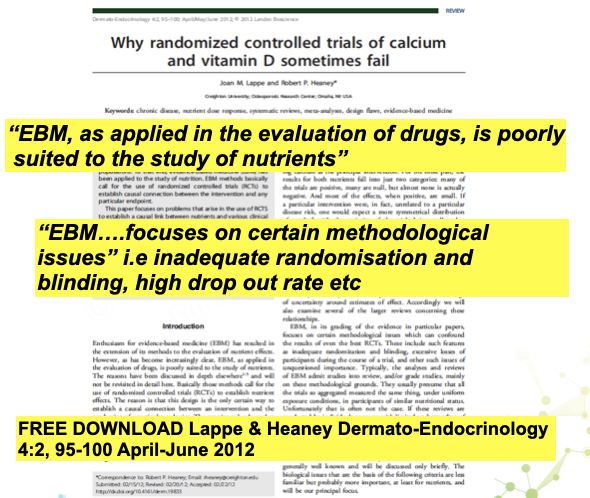
Strange as it sounds, the people doing the research and certainly the ones doing the meta-analysis do not always understand at a deep level the biology of what is being studied.
I would also suggest again, that they are looking at it all through the “lens” of medicine/drugs and simply do not understand that humans are highly complex biological systems that are highly interconnected.
With a drug, the root cause of something doesn’t always matter, you can suppress a system or symptom with a drug.
When you are giving a nutrient that is missing, you need all the other nutrients (proteins/fats, vitamins and minerals) to be present in adequate amounts or the pathway/system will still not work properly, and the nutrient is deemed unnecessary or ineffective.
See below the pathway for serotonin and melatonin.

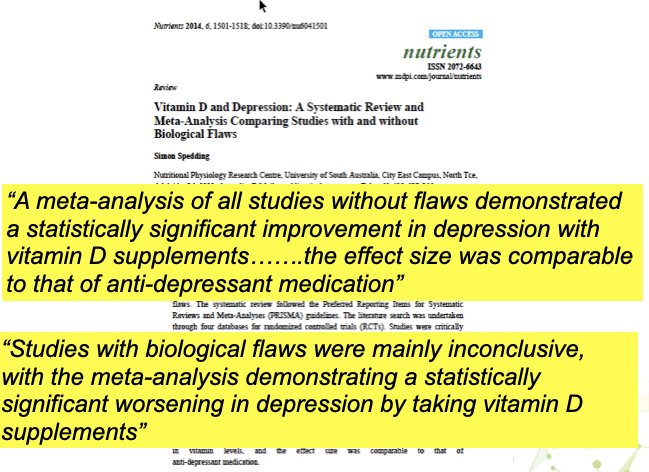
So, with vitamin D for depression, there were huge issues with some of the studies being analysed.
Thus, they do the analysis with the flawed studies included and without.
Without the flaws:
- they were diagnosed deficient
- they got optimal doses and were re-tested over 100nmol/L
The results showed vitamin D was comparable in efficacy to anti-depressant medication.
But when they included the studies with flaws, the results suggested a statistically worsening effect by taking vitamin D supplements ????
Maybe your patients are diagnosed and given good doses up to optimal (over 100 nmol/L) and still do not respond.
Maybe that is because they are low in magnesium, the mineral that is needed to turn vitamin D into the active metabolite that controls inflammation.
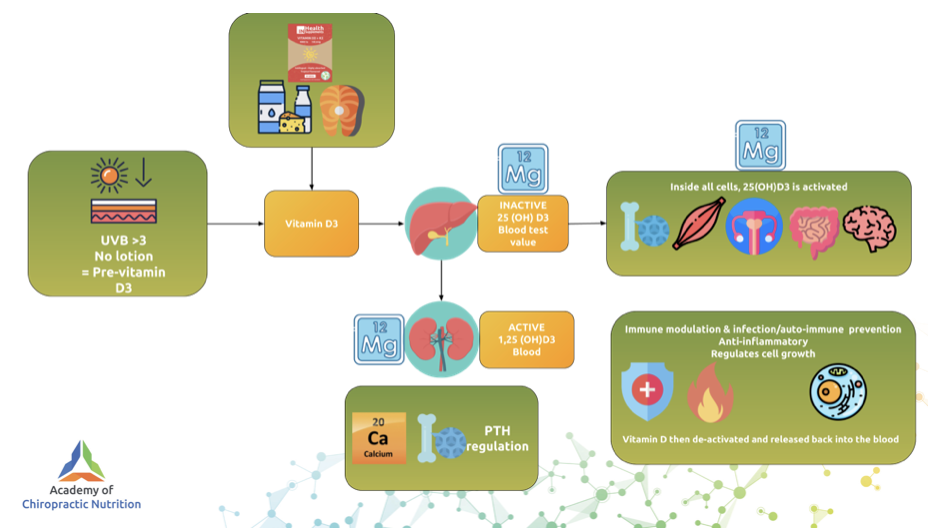
FYI, this is known as “Magnesium dependent vitamin D resistant rickets”

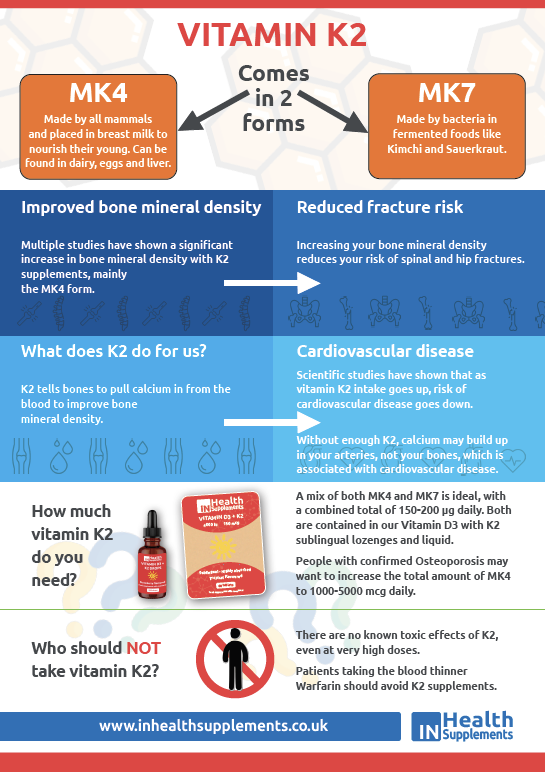
Maybe they are low in vitamin K2 and that has allowed excess calcium to build up in their arteries and lead to heart disease?

Let us get back to basics and some common sense.
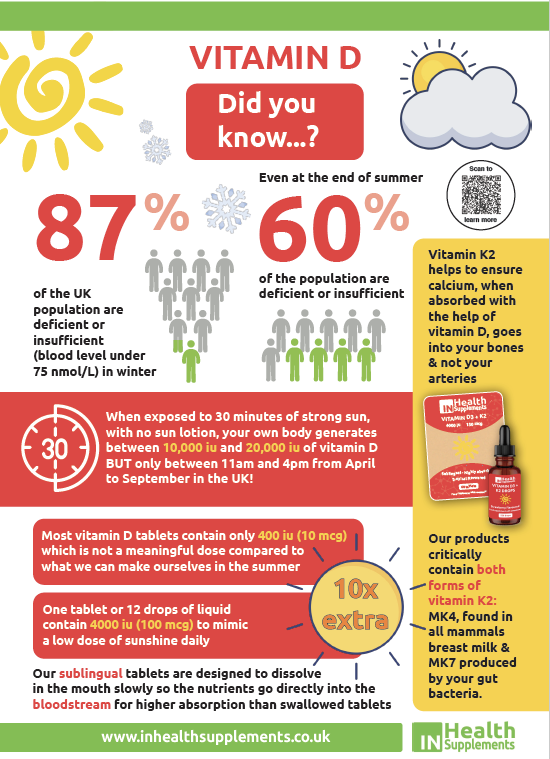
They recommend 400 iu (10 mcg) daily, but from food not supplements.
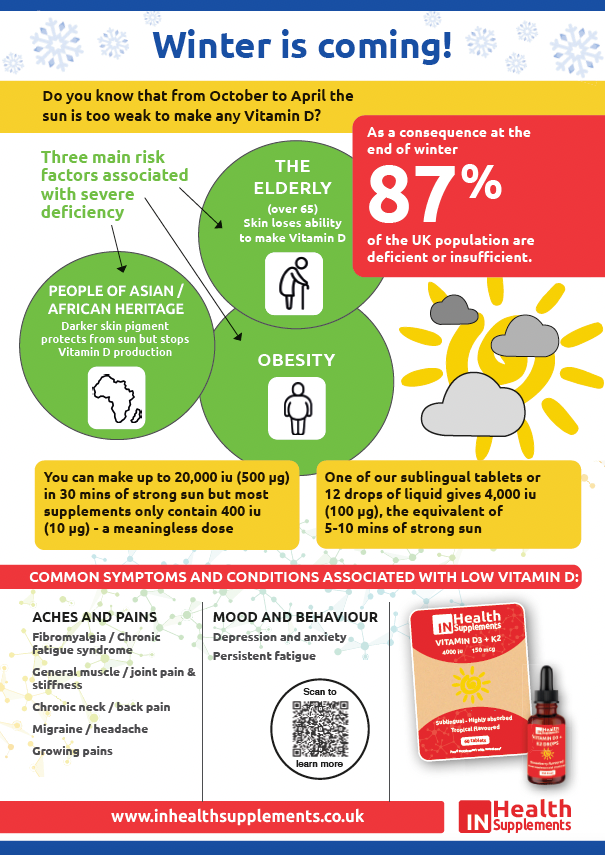
So, let’s remind ourselves how much we can make in full body exposure, because that might inform us about supplementation levels when we cannot get it from sunshine, which is October to April in UK.
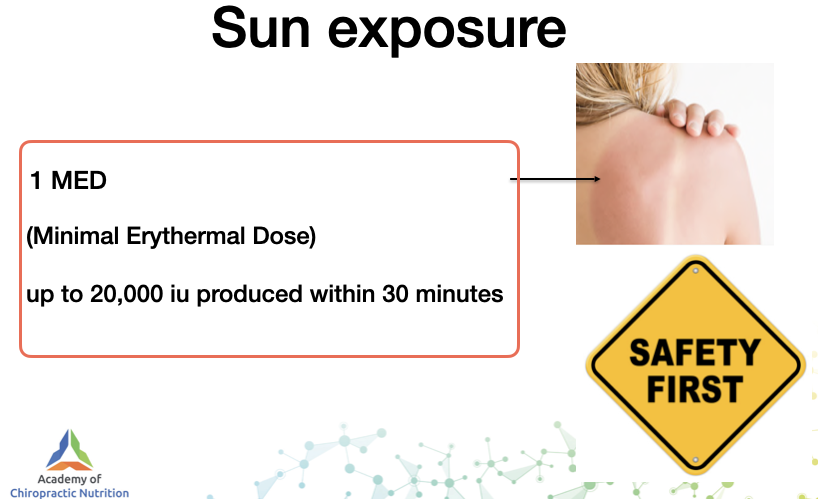
Up to 20,000 iu with 1 MED (whole body exposure until pink), this will vary between people and those with darker skin.
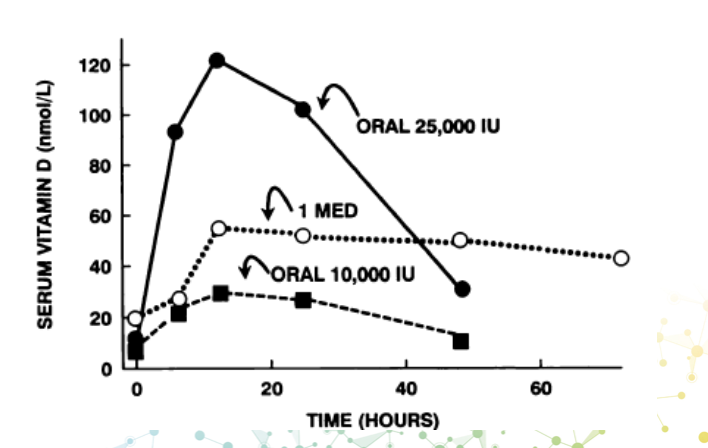
And you can compare 1 MED to 10,000 iu and 20,000 iu oral dose.
I think that fact alone should make the suggestion that we only need 400 iu daily (and get it from food) laughable.
But let’s take it further.
You cannot get too much vitamin D from sunshine, your skin simply turns off production.
So, if we take people that live in a sunny climate year round and work outdoors, we can get a good idea of what optimal endogenous production would give us in terms of blood levels.
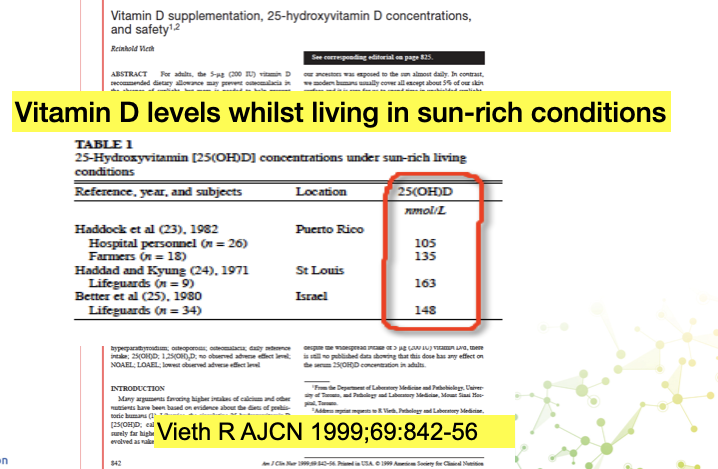
So if your body, which regulates your endogenous vitamin D levels via skin production, can keep the levels in the 100’s, why are the NHS/Tim Spector happy with 30 nmol/L?
And the answer is the poor quality studies as discussed above seen through the lens of “medicine” and the aim to make vitamin D a silver bullet drug, that stop cancer on its own.
As we saw, the studies are poor and, in reality if you are optimal in vitamin D but have a terrible diet loaded with ultra-processed foods, you are still very likely to get cancer.
The reality is deficiency as defined as under 50 nmol/L is present in 40% of the general population at the end of winter, but we include 50-85 nmol/L as insufficient then it is 87%.
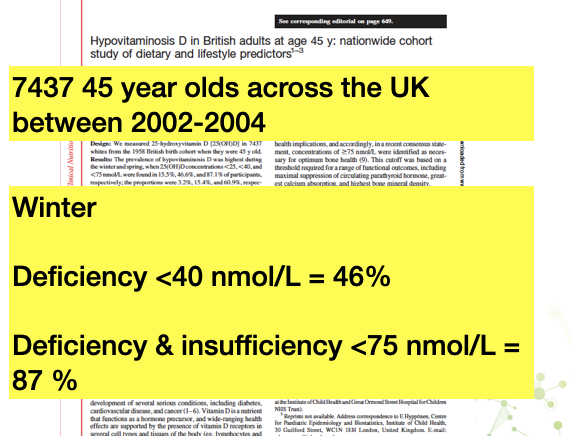
Note the three high risk groups for severe vitamin D deficiency are: Elderly, obese, and non-caucasian.
Those groups the rates are 100%.

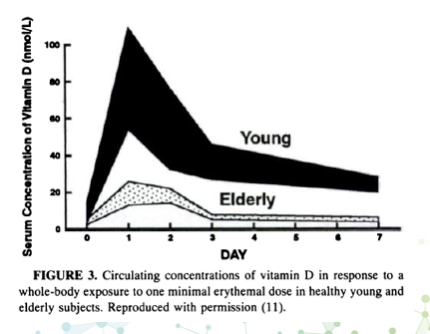
See below, by the time you are 65 years old your skin just doesn’t make vitamin D like it used to.
Why is 50-85 nmol/L insufficient?
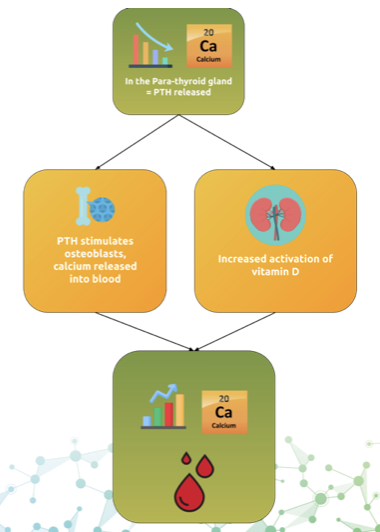
Because if you go from 50 to 85 nmol/L then you absorb 65% more calcium from your diet.
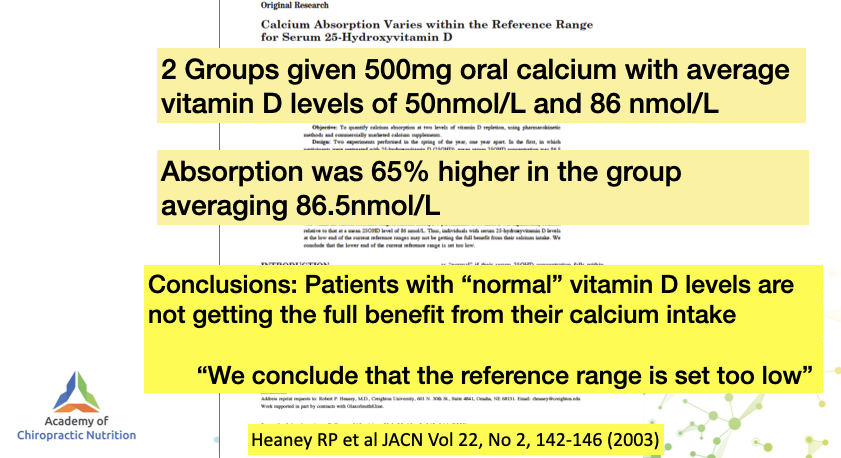
And your para-thyroid hormone (PTH), the one that tells your bones to mobilise calcium into blood, is maximally supressed.
All the information you need to educate patients is found in our infographics which you can order free of charge from inhelathsupplements@yahoo.com