We are soooo close now to Turmeric PLUS hitting your clinics, they are now being whisked off to be put into pouches as we speak and will be within 2 weeks, sorry I cannot give a specific date.
Last Wednesday we went over the B12 Protocol live, below is a recording for you.
Passcode: JYXt3e5.
(note the full stop at the end is part of the password).
FYI, in 2025 we will be launching blood testing as part of our company.

And one test that I am going to be using a lot more in clinic is two parts of the iron panel.
- Serum Iron: This is the amount of iron in the blood, circulating freely while bound to transferrin
- Ferritin: Your iron reserves for when blood runs low
Serum iron is like a current account and ferritin is like a saving account. When your current account runs low, you top up from the savings account.
But equally, if you have excess, then you stick it in storage, which is ferritin.
The challenge is, if your iron gets too high it can be very, VERY inflammatory and reactive.
Not to get too nerdy here, but, iron/Fe 2+ reacts with oxygen or hydrogen peroxide, to create a HYDROXYL radical.
This is known as FENTONS reactions.

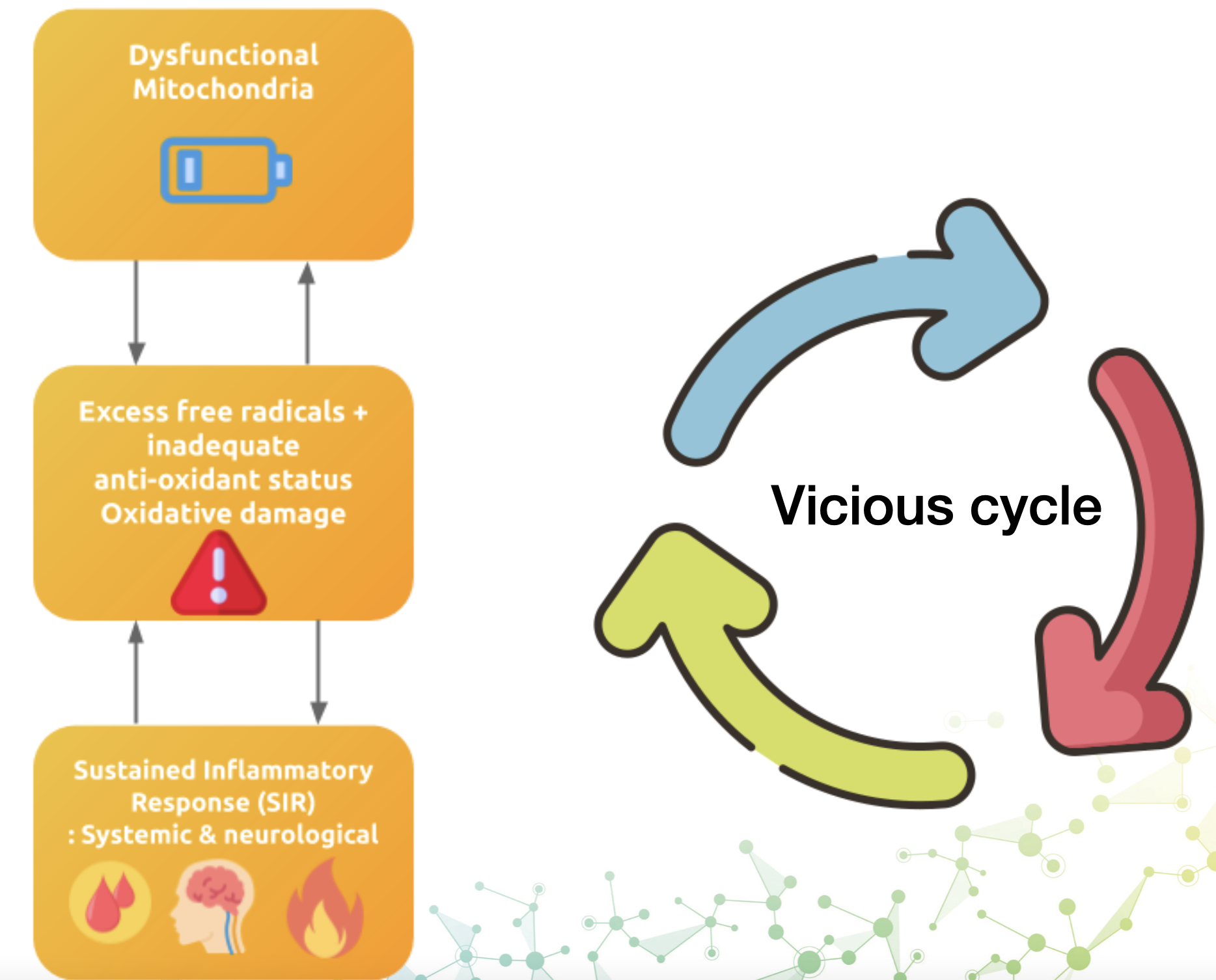
The bottom line, HYDROXYL radical is a highly powerful free radical which creates massive OXIDATIVE DAMAGE.
Thus, my friends, iron overload will shorten your life via cancer, strokes, diabetes, CVD and more.
It is also related to osteo-arthritis.

Note one of the conditions on the list was diabetes.
Now association is one thing, and is useful, but ideally, we want some intervention.
Let’s see what happens when a group of patients with metabolic syndrome (insulin resistance, glucose intolerance and obesity), are bled twice for a total of between 550 and 800 ml of blood and reassessed at four weeks.
Now note that at the assessment none of the patients would be anywhere near the level to be classified as iron overload.
The two groups were between 173-188 ng/ml.
In the UK, GP’s are not going to be concerned unless you hit at least 400 ng/ml.
We, on the other hand, want it under 100 but not lower than 50.

And note, if you give blood, they will take 500 ml of blood, every 3 months.
The results are impressive.
Note SPB = Systolic blood pressure
HOMA – Is a combination of glucose and insulin markers
Yellow is blood removal, red is control group.

These are clinically meaningful changes, with zero diet changes.
A drop in systolic blood pressure from 148 to 130 is the difference between the GP prescribing or not.
Glucose 11% drop.

Note, a fasting glucose of over 100 mg/dl (5.6 mmol/L) is considered PRE-DIABETIC.
Thus the GP would de-classify them from pre-diabetic to normal after 2 two blood draws.
Diastolic BP 10% drop.

And of course, ferritin, now down to just above 100 ng/ml in the blood draw group, but staying at an NHS normal 149 ng/ml, which even I find surprising given the difference between the two outcomes.

This shows just how damaging iron accumulating in your tissues is.
Let that data settle into your brain, you can go from pre-diabetic and hypertension to normal with two simple blood donations.
In 2025, we will start the blood testing and a new course on functional blood testing for neuro-mechanical practitioners – you and your patients are going to love it.