We have some exciting news today about how you can educate your patients.
We now have the ability to directly email patient videos on each product from your IN Health account, and it is simple.
Once you are LOGGED IN as a PRACTITIONER, then on the far right of the navigation bar, you will see a tab SHARE VIDEOS.

Clicking that takes you to a separate page with currently eight videos (with more pending).
Note at the bottom of each video is a little box to tick “SHARE THIS VIDEO”
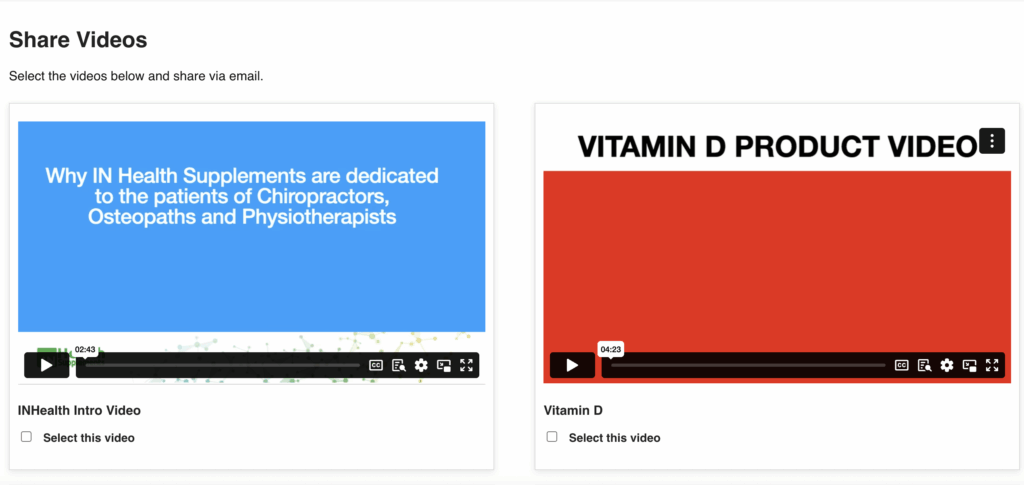
Simply click on the ones you want your patient to view, usually the product being sold AND if it is the first time, ALWAYS send the INTRO to IN Health supplements video.
Then, at the bottom, fill in your name and email, my browser does this for me automatically when I click on it, and then add patients’ email.
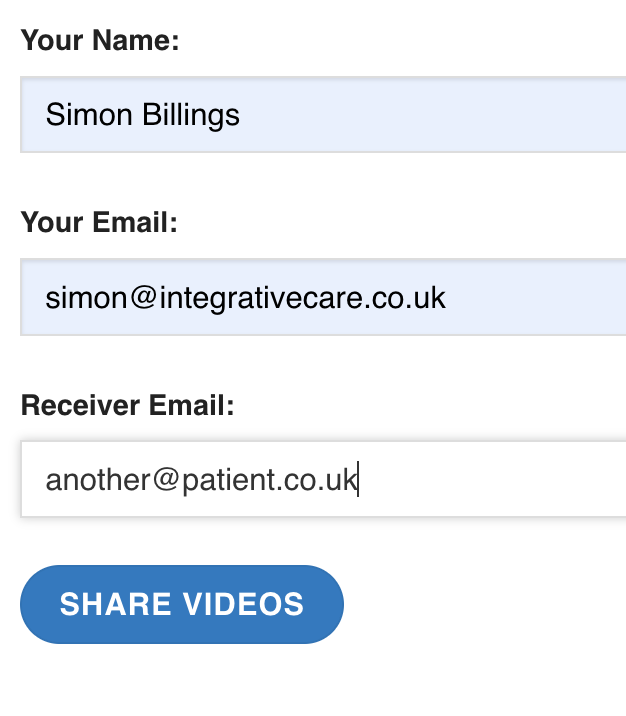
Click “SHARE VIDEOS”, and they instantly get to their inbox:
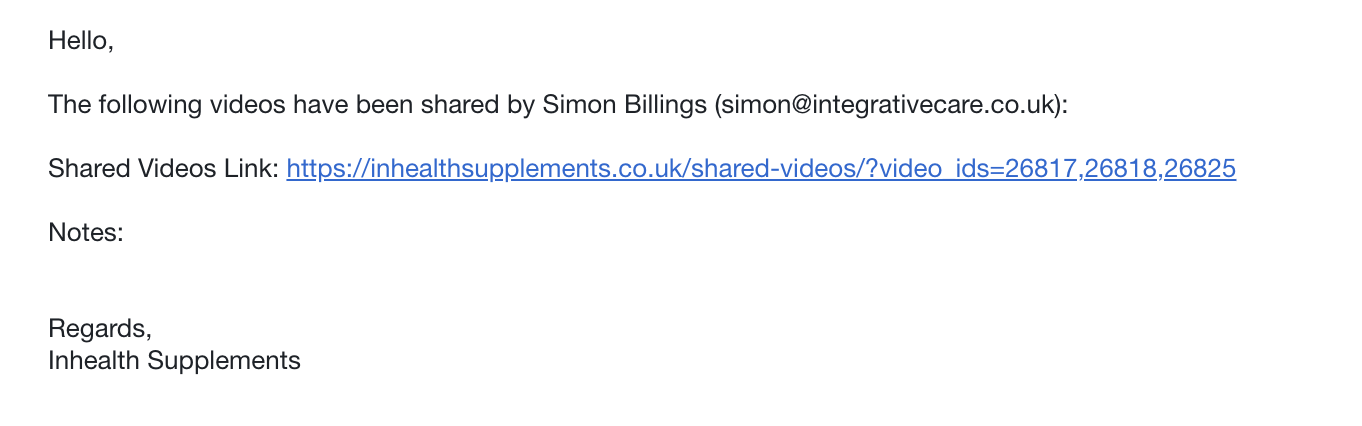
They click the link, and it takes them to a bespoke page with ONLY the videos you selected, in this case IN Health INTRO video, Chiro Ice and COLLAGEN.
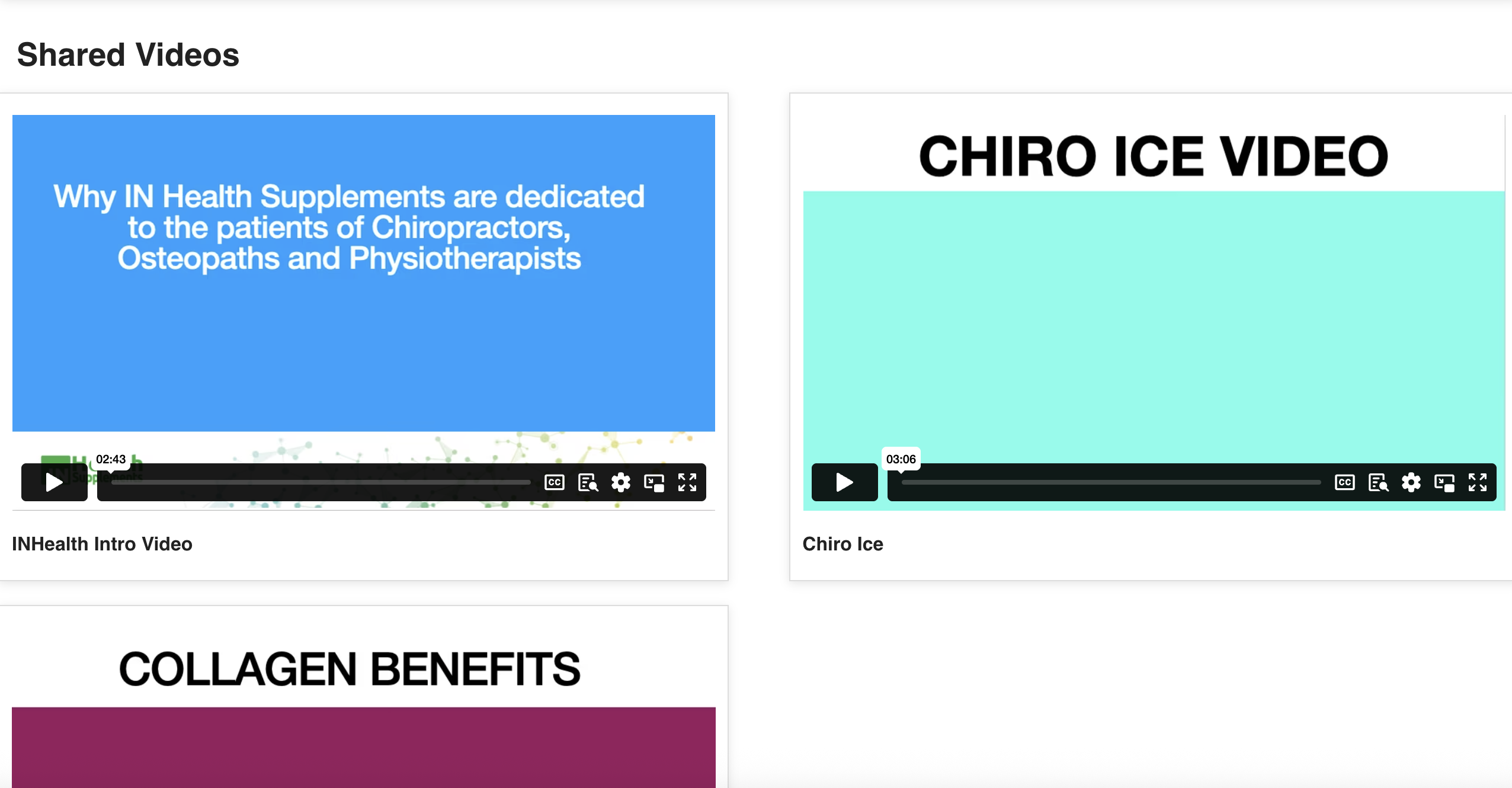
It is that simple.
Even simpler, get your reception/CA to do it.
I would recommend they always keep the IN health site open and logged in and when the patient buys the first time, send the INTRO video and appropriate video for the supplement.
Let me explain why the INTRO video is so important.
From a patient’s POV a supplement is a supplement, and the nuance of what nutrients are in the pouch, the dose and the form are lost.
If they do not understand why we are different and selling CLINICAL GRADE supplements, they will buy once and then buy next time in a supermarket or on Amazon.
We are specialists in supporting your care.
That is the point.

We get results with optimal doses.
These are bespoke formulas. I could have had generic formula like vitamin D and K2 in a capsule in a bottle in no time for far less cost and made far more money.
But I have three things that mean we can make a unique supplement range:
I have years of experience at the coalface working for results, plus years of running tests on patients to see patterns.
And I have read the literature DEEPLY.
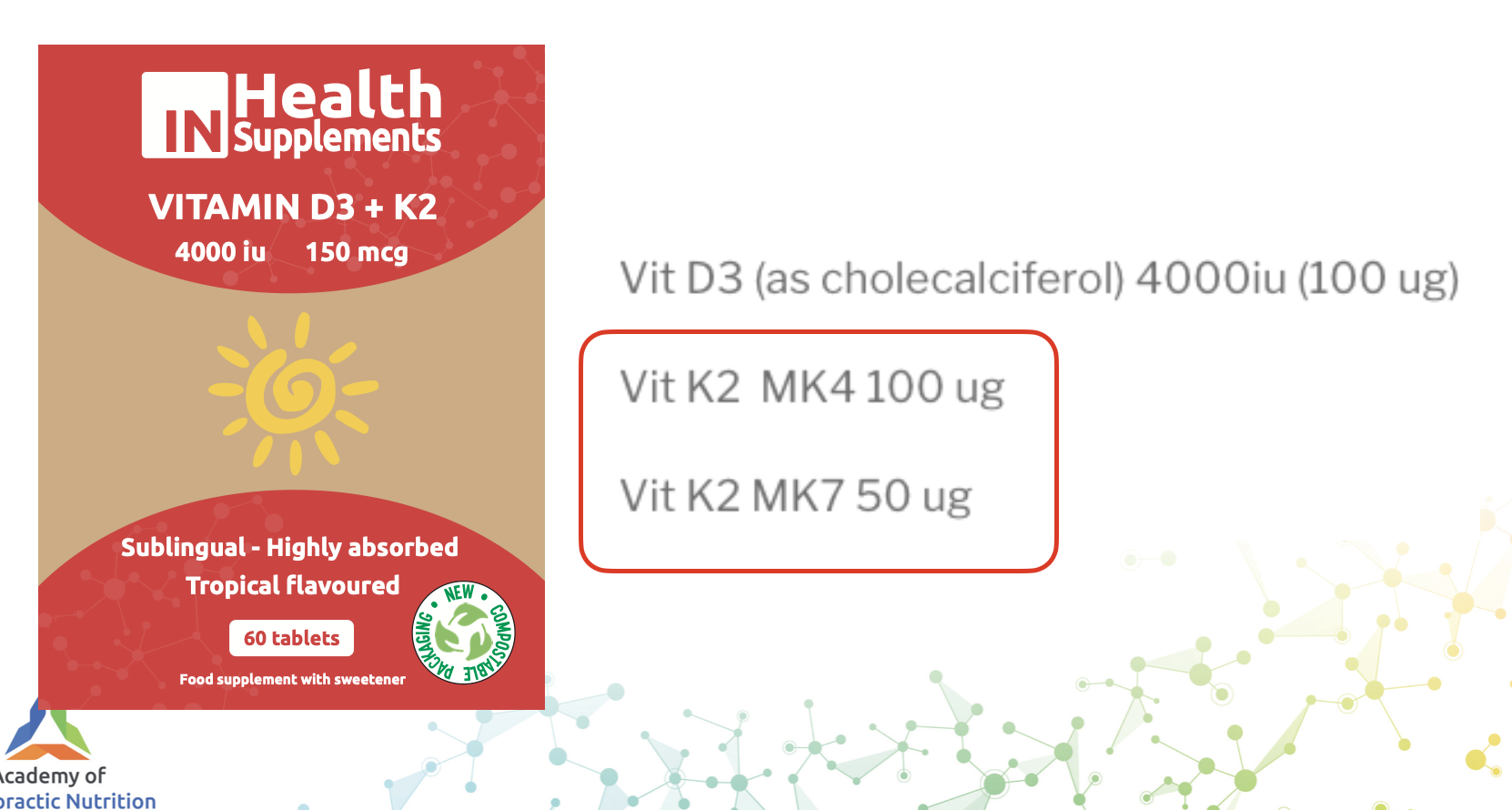
For example, we use a blend of two forms of K2, MK4 and MK7, while 99% of companies use MK7 only and that is an issue. Here is why.
Your body makes MK4 from K1 and MK7, which makes you think maybe MK4 is pretty important 🤔
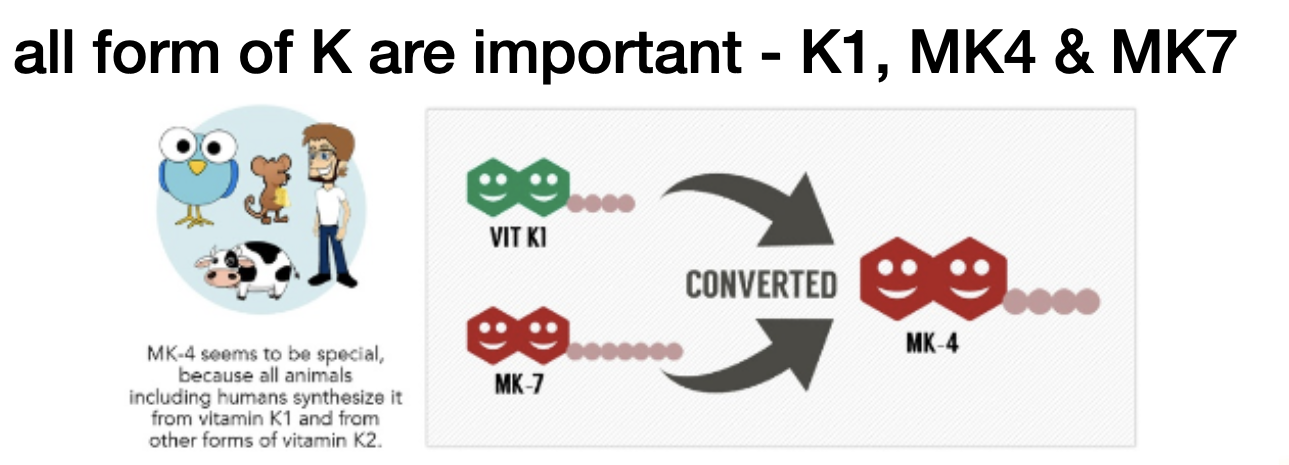
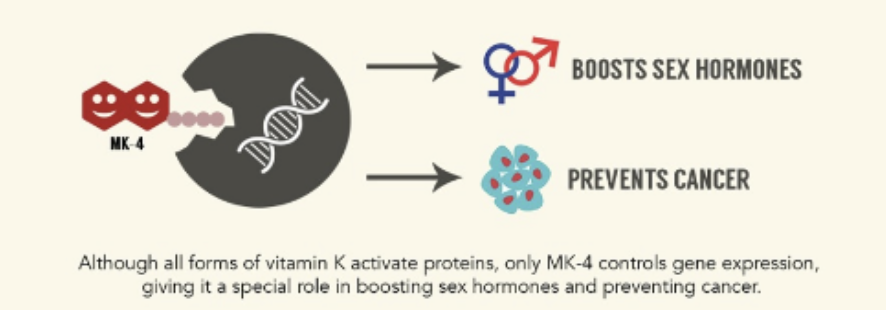
And MK4 does a lot more than just bones.
In fact, every single mammal makes it and puts it into its breast milk – think about that.

Hence, why grass fed dairy (milk from a mammal) is a great source of K2 in the MK4 form but not MK7.
MK4 also crosses the placenta but MK7 does not (at least in any significant amounts).
Again, think about that from an evolutionary POV.

So, riddle me this, do you want your K2 in the blood, floating around, or in your cell (bones and more) doing the business?

The 4 in MK4 is related to the side chain, and this is what makes it so bioavailable to the CELL, and hence it has a short half life in the blood.
Ironically, MK7 is less bioavailable to the cells, which makes it hang about in the blood longer and aka has a longer half life.
And it is that manufacturers try to tell you makes it better than MK4.

Having read the literature, here is the truth, the majority of studies done to let us know K2 is so good for bones is done using MK4:

There are more MK7 studies coming, and in reality we want both.
I would suggest as MK7 is converted to MK4, it is used by the body as a slow release / back up for MK4

Hence, we use both, totally 150 mcg, if you are using another brand I suggest you check the dose (it will be less than 150 mcg) and the forms.
A nutrient dense diet would give you around 200 mcg of K2 in a mix of forms.
And that is why we also added 50 mcg of K2 MK7 to our One a day Essential Multi, to make it a total of 200 mcg in a 50:50 split of MK4:MK7, mimicking a great diet.
That is nuance, that is DEEP understanding of the literature.
We understand the CORE CONCEPTS that drive patients ill health:
And the results are:

Let us get into the big stuff, dosing.
The RDA/RI for vitamin B6 is 1.5 mg but clinical studies use up to 100 mg.
Example as per below for PMS and depression:
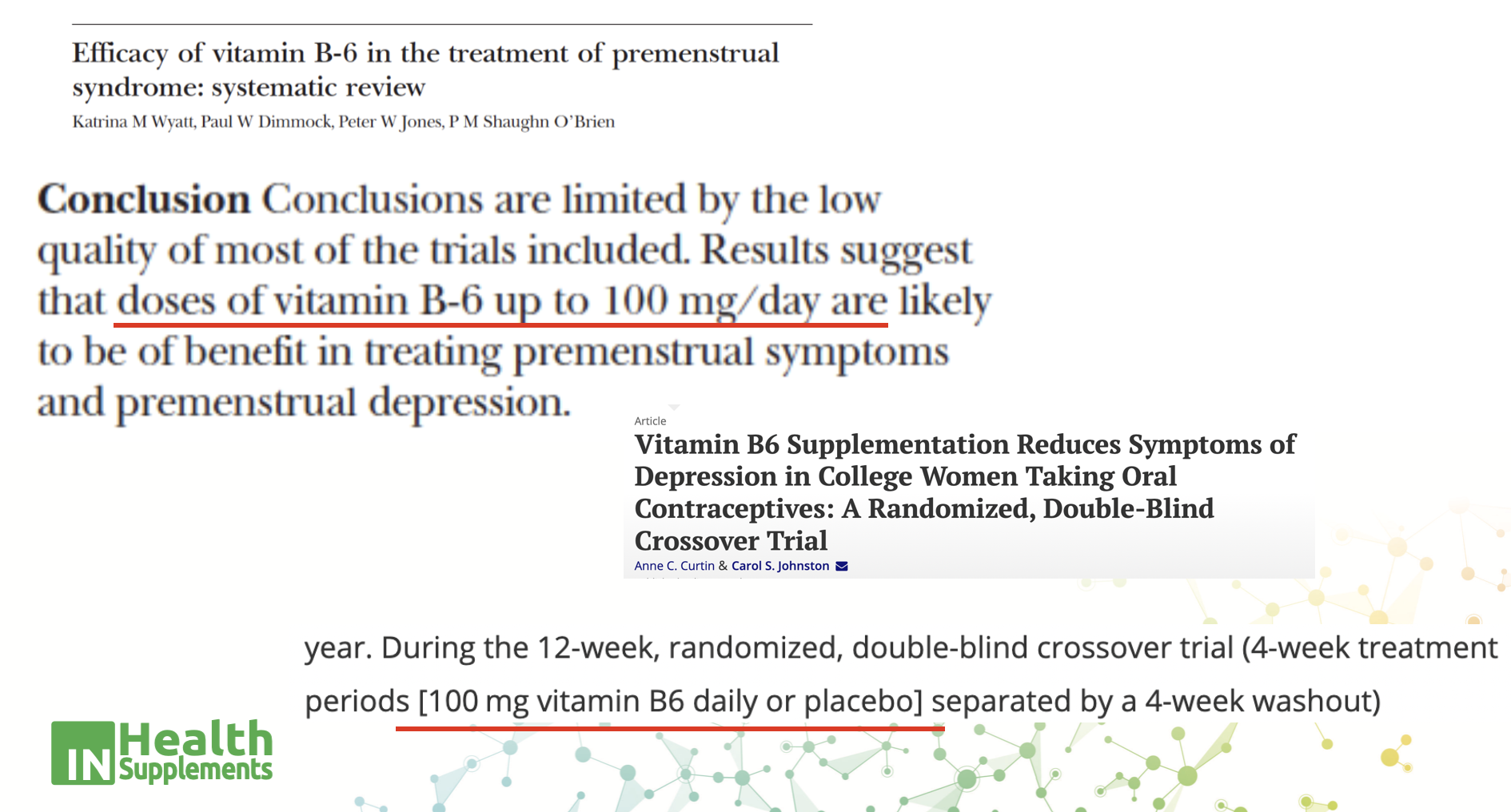
If the study uses 50-100 mg of B6 for improving PMS or depression or pain etc, then using 1.5 mg or even 10 mg isn’t going to work.
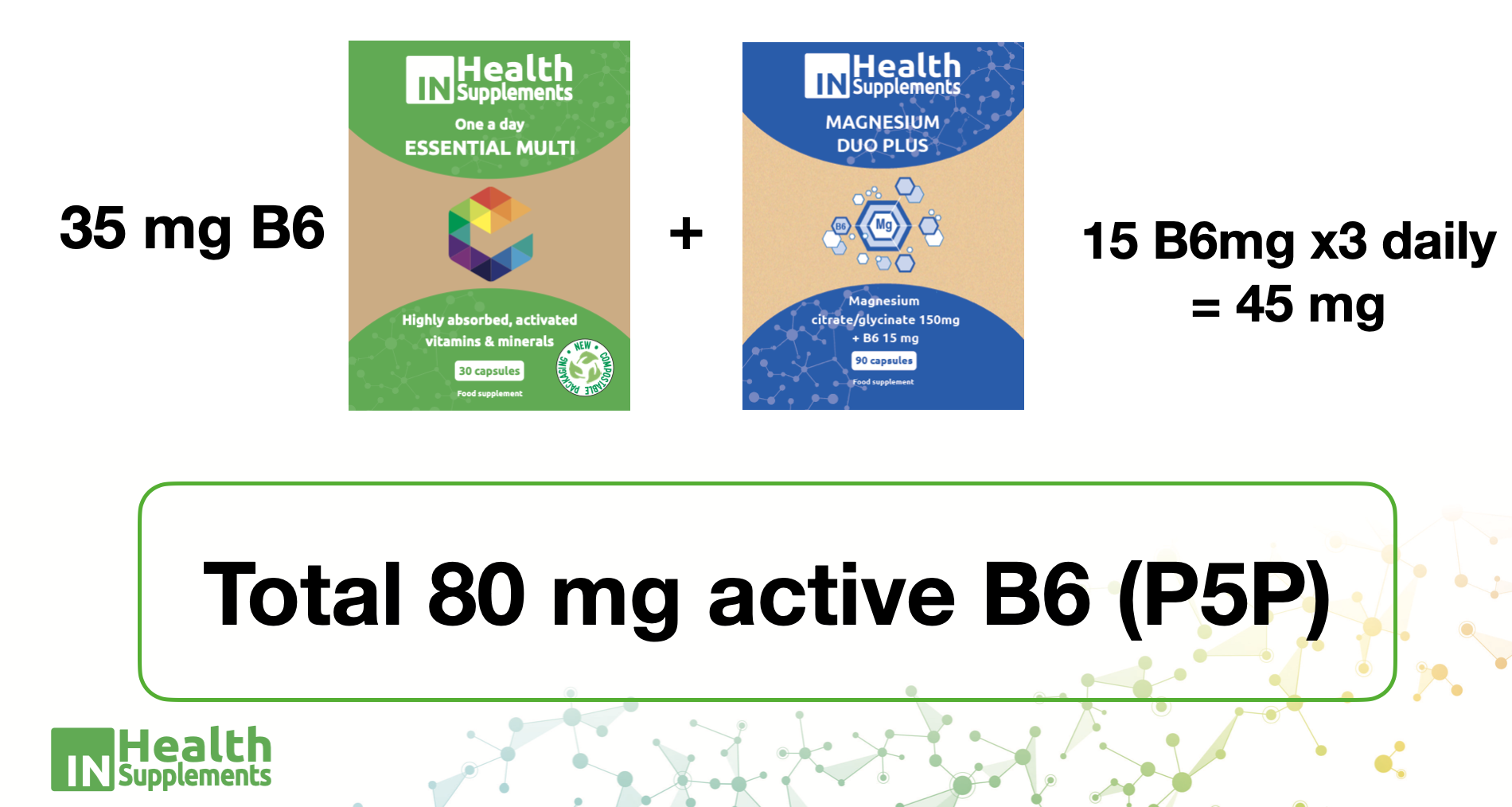
That is why we have 35 mg in our One a day Essential Multi and 15 mg per capsule of the Mag Duo PLUS, totaling 80 mg if using the full dose of magnesium of x1/3 daily.
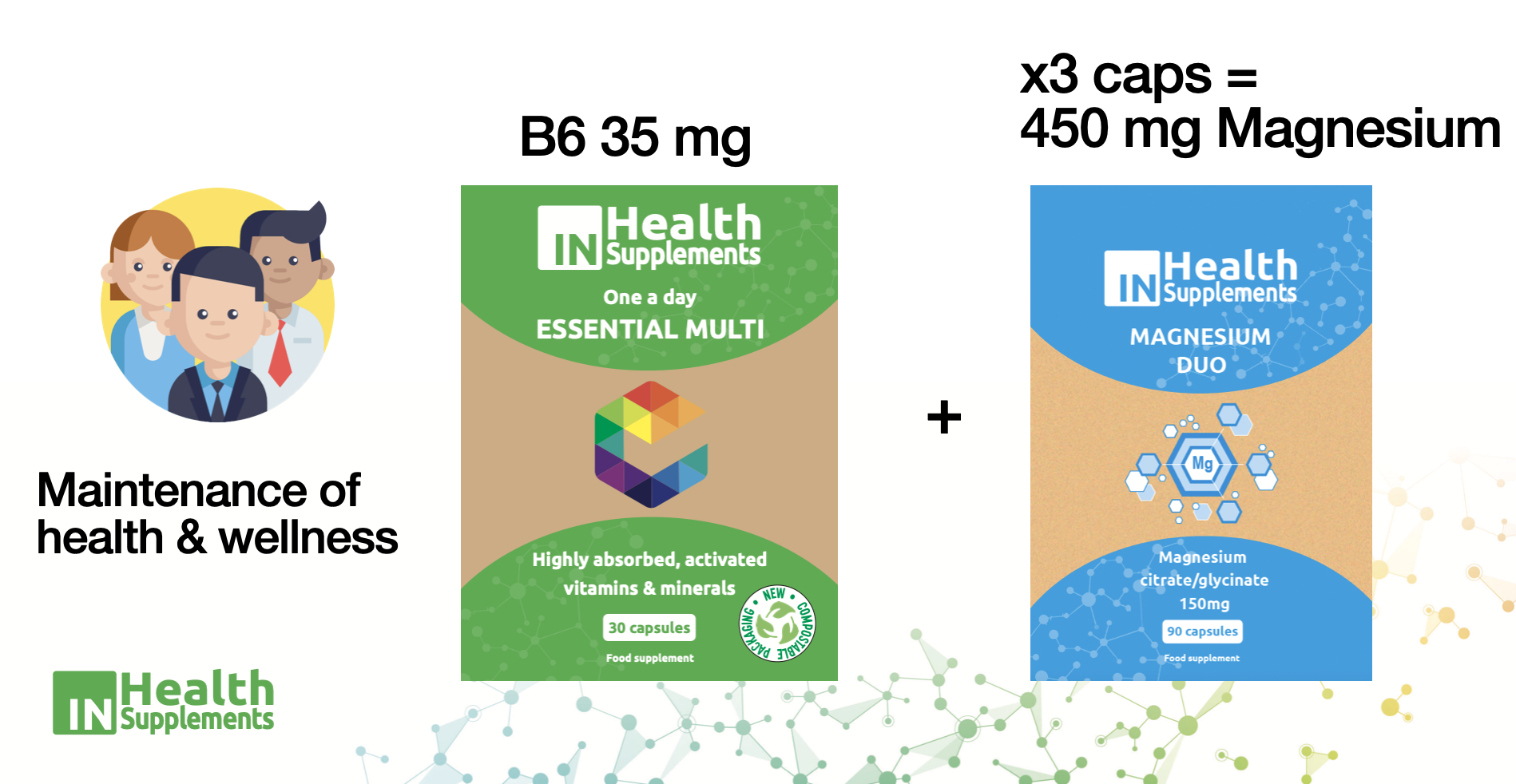
If your patient doesn’t have PMS or depression or chronic pain etc, then just use the One a day Essential Multi with Mag Duo, which does not have any B6 added, for a lower dose of 35 mg.
Then we need to consider active forms of nutrients vs inactive.
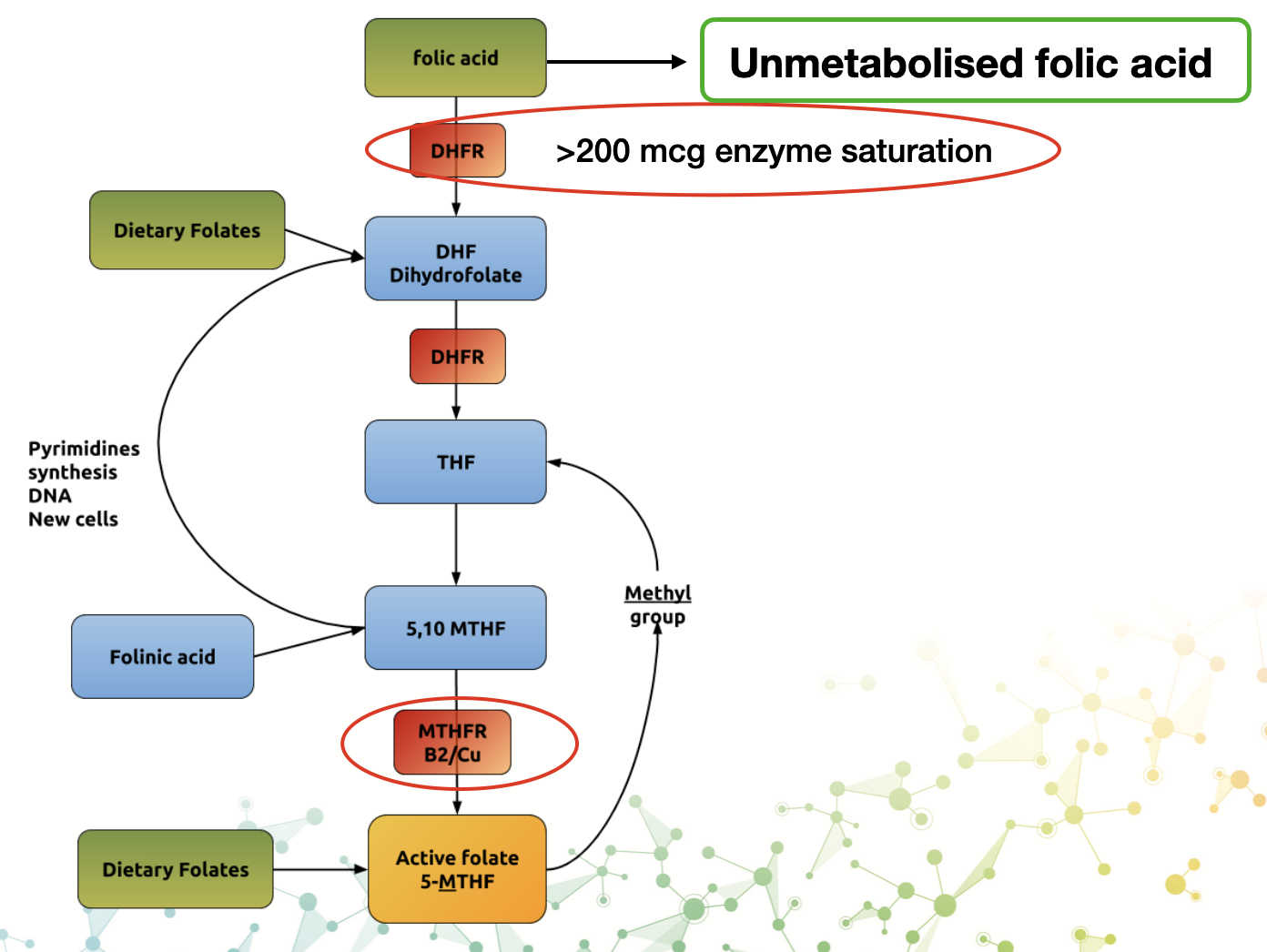
Folic acid is an inactive man-made substance, it does nothing.
It must be converted through a series of chemical conversions to the active metabolite, METHYL FOLATE or 5MTHF.
The issue is that the conversion is limited by enzyme saturation and genetic issues.
In addition, all our supplements with active/methyl folate are being switched to the patented and proven form of

You can check them out here:
https://www.youtube.com/@Quatrefolic
These are real differences that make the difference between taking supplements because they are “good for you”, and using our CLINICAL GRADE supplements with OPTIMAL dose, in ACTIVE forms, that make the patients feel the difference.
If you simply send your patients the INTRO video all of this is explained in 2 minutes 43 seconds.
– Watch the INTRO VIDEO below so you know what they are getting.
Click it 👇
